Key takeaways
Twin reversed arterial perfusion sequence happens only when babies share a placenta
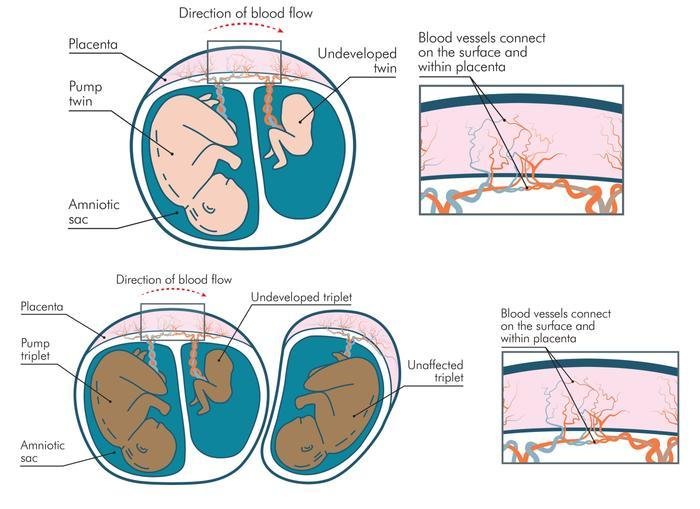
One baby develops normally while a non-developing baby still receives blood through shared vessels
The developing baby’s heart can become strained, so close ultrasound monitoring is essential
Specialist treatment, often laser therapy, can protect the developing baby and improve outcomes
Understanding twin reversed arterial perfusion sequence
Twin reversed arterial perfusion sequence is a very rare condition that can affect monochorionic twin or triplet pregnancies, where your babies share one placenta.
In TRAPS, one baby develops as expected, while the other baby does not form properly but still connects to the placenta through blood vessels. The non-developing baby may grow in size but will not look like a fully formed baby and cannot survive on their own.
Because of these connections, the developing baby pumps blood for both their body and the non-developing baby, whose body cannot survive outside the womb. Over time, this extra work strains the developing baby’s heart and, if untreated, may lead to heart failure or loss.
TRAPS is usually picked up on specialist ultrasound scans, rather than through symptoms you notice yourself. This is why attending every scan you’re offered is so important.
Health risks and signs to look out for
TRAPS only affects pregnancies where at least two babies share a single placenta, known as monochorionic pregnancies. It happens in about one in one hundred of these pregnancies. Pregnancies where each baby has their own placenta, called dichorionic or trichorionic pregnancies, are not at risk of TRAPS.
Most people carrying twins, triplets or more with TRAPS do not notice any clear symptoms. The condition is usually only visible on ultrasound, so regular scans are vital.
In more advanced cases, too much amniotic fluid, called polyhydramnios, can build up and cause symptoms similar to Twin-to-Twin Transfusion Syndrome (TTTS) (LINK - Inf 16).
You should contact your maternity team urgently if you notice:
- Sudden weight gain or your bump becoming much bigger within a day or so
- Feeling breathless at rest or having palpitations
- Your tummy feeling very tight, uncomfortable or looking stretched and shiny
- Increased thirst, early contractions or new back or leg pain
TRAPS can also increase the risk of preterm labour. Labour may start on its own, or your doctor may recommend an earlier birth if that’s safest for your developing baby.
Don’t miss what matters
Get Twins Trust news, support updates and practical resources—straight to your inbox.
Treatment options and monitoring during pregnancy
Because TRAPS is rare, if you’re diagnosed you should be referred to a specialist fetal medicine unit experienced in complications of twin and triplet pregnancies. Your team will look at how far along your pregnancy is and how well the developing baby’s heart is coping before recommending a plan.
If TRAPS is found later in pregnancy and the baby’s heart looks healthy, doctors may recommend close monitoring with frequent scans rather than immediate treatment. When TRAPS is diagnosed earlier, treatment is more often needed to protect the developing baby.
The most common procedure is laser therapy, which blocks the umbilical cord of the non-developing baby and stops blood flowing between the two. This reduces the strain on the developing baby’s heart and usually allows them to grow more safely for the rest of the pregnancy.
Laser therapy is done under local or spinal anaesthetic, so you’re awake but your tummy is numb. The doctor passes a thin needle and hollow tube through your abdomen into the fluid around the non-developing baby. They then use a tiny telescope and laser fibre to seal the blood vessels in the umbilical cord.
After treatment, you’ll have regular follow-up scans so your baby’s growth and heart function can be checked closely. Your team will talk you through the risks and benefits so you can make informed decisions together.
Planning birth and looking after yourself
Your maternity and fetal medicine teams will talk with you about the safest way to give birth, based on your baby’s health and your situation. If your baby is well and there are no other concerns, vaginal birth may be possible. If there are worries about your baby’s condition, a caesarean birth may be recommended.
After your developing baby is born, you’ll also deliver the non-developing baby and any remaining tissue, which often shrinks in size after laser treatment. Your team should explain clearly what to expect, and you can ask them to go over things as many times as you need.
Hearing that one of your babies will not survive is devastating, and it’s normal to feel shock, grief, anger or guilt. None of this is your fault, and you deserve support while you look after yourself and your developing baby.
Try to eat well, stay moderately active, rest when you can and make it to all your appointments and scans. Our pregnancy tracker (LINK - antenatal care checklist) can help you keep on top of the checks and tests you should be offered throughout pregnancy.
If you notice new symptoms or you’re worried at any point, contact your midwife, doctor or triage unit for advice. Reaching out early means your team can check you and your babies and plan the best possible care.
Supported by the GIFT-Surg international research project which is funded by the Wellcome Trust and EPSRC.
Published